
INTRODUCTION
Hypertension is the third cause of death in Indonesia, and the prevalence of hypertension, based on the Indonesian Basic Health Research 2018, was 34.1% (Ministry of Health of the Republic of Indonesia, 2019). The 8th Joint National Committee described that hypertension can be treated by either a single therapy or a combination. The first drugs of choice are calcium channel blocker (CCB), diuretics, angiotensin-converting enzyme inhibitors (ACEi), and angiotensin receptor blocker (ARB). ACEi is rarely used due to its intolerance, e.g., dry cough, fatigue, headache, and sudden drop of blood pressure. ARB, however, is the best choice as a single therapy or in combination (Abraham et al., 2015). The use of CCB, which had been proven to be related to the prevention of cardiovascular disease, as compared to ARB, resulted that CCB therapy showed the better outcomes than ARB (Black, 2004; Wu et al., 2014). However, both the CCB and ARB indicated similar effects on mortality and heart failure (Wu et al., 2014).
The treatment of hypertension should be safe and does not interfere with the quality of life (QoL) of the patients (Fletcher, 1999). Based on the trials of hypertension prevention and the treatment of mild hypertension, it was shown that a decrease in blood pressure was directly proportional to the improvement of the QoL (Batey et al., 2000; Grimm et al., 1997). The QoL can be determined by assessing the physical, mental, and social welfare conditions of the patients using the Euroqol 5 dimensions 5 levels (EQ5D5L) and Euroqol visual analog scale (EQVAS) (EQVAS/patient’s self-health assessment). EQ5D5L is a generic and general instrument that aims to measure, compare, and assess health status in all the types of diseases (Devlin and Brooks, 2017). It includes five dimensions: mobility, self-care, normal activity, pain/discomfort, and anxiety/depression. Each dimension has five levels: no problems, few problems, moderate problems, severe problems, and extreme problems (Herdman et al., 2011). These assessments can help to manage therapy in patients with chronic conditions and contribute to an evaluation of primary care services (Bakas et al., 2012; Hand, 2016).
This cross-sectional study was conducted to determine the QoL of the hypertensive outpatients treated with a single therapy of CCB and combination of CCB and ARB at a primary referral hospital in West Java, Indonesia. Measurement was conducted using the validated-EQ5D5L and EQVAS questionnaire from December 2018 to February 2019.
MATERIALS AND METHODS
Design
A cross-sectional study was performed on adult hypertensive outpatients (aged 18–60 years) at a primary referral hospital in West Java, Indonesia. Inclusion criteria were as follows: 1) patients were diagnosed with code ICD10-CM-I10 (ICD-10 is a specific code for primary hypertensive patients who do not have comorbid heart or kidney disease) (Beckman, 2014), 2) patients were treated with ARB and/or CCB either in single therapy or in combination for more than 6 months, 3) patients agreed to participate in this study by signing the informed consent, and 4) patients did not suffer more than one comorbid disease. Exclusion criteria were as follows: 1) patients did not continue their health control or did not respond to the scheduled-health control and 2) patients passed away during the study.
Patients
Participants were 83 hypertensive outpatients, comprised of 59 female and 24 male. The minimum sample size was calculated using an unpaired categorical equation:
with a type 1 error value of 5% (Zα = 1.96) and type 2 error value of 20% (Zβ = 0.84), and the precision of the previous study was 0.24 as described previously (Sari, 2017).
or minimum sample size of 23 patients.
All 83 outpatients, who had received antihypertensive drugs for 20 ± 3.3 months, were included in this study.
Ethics statement
The study had been approved by the Hospital Ethics Committee (approval document No. 445/065/TKEP/2018) and was conducted in accordance with this ethical consideration. The patients’ privacy, confidentiality, and security were maintained for limited access only. An informed consent had been signed before the study was conducted.
QoL instrument
The QoL was assessed using the EQ5D5L and EQVAS (visual analog scale/patient’s self-health assessment). This instrument had been validated (Setiawan et al., 2018), tested, and retested for its Indonesian version (Staff, 2018) and resulted from available value sets (Purba et al., 2017). Higher scores indicate a better HRQoL.
Statistical analysis
Patients’ demographic information (e.g., blood pressure, age, sex, education level, occupation, marital status, ethnicity, tea and/or coffee consumption and smoking, physical activity, comorbidities, and daily antihypertension drugs that were taken) was analyzed using the descriptive analysis. The bivariate analysis was used to see the relationship between the independent and dependent variables. The level of significance used was 5% (p ≤ 0.05 means that there is a correlation between the two variables) followed by multivariate analysis, e.g., multiple logistic regression analysis for categorical independent variables and two categorical dependent variables. All analyses were carried out using the SPSS version 22.0 (SPSS Inc., Chicago, IL).
RESULTS AND DISCUSSION
The age of the patients was 51 ± 1.04 years, 59 (71.3%) were female, 70 (84.3%) were married, and 55 (66.2%) never undertook physical activity. Daily drugs consumed were 4 ± 0.19 items and the length of hypertensive treatment was 20 ± 3.3 months. Majority of the patients were Muslims (95.2%). The lowest QoL belongs to hypertensive patients with primary education level. These patients show a limited knowledge about the antihypertensive drugs, and some of them even admitted that they sometimes forget to take their medication. The result was compared with that of Skevington, who studied cross-cultural data taken from 9,404 sick and well adults in 13 countries. This author reported that there was a positive and sequential increase of environmental QoL from no education to tertiary education. The patients with higher educational level indicated better feelings, less dependence on medication and treatment, and positive perceptions of financial resources (Skevington, 2010).
Moreover, 42.2% of the patients routinely drink tea and/or coffee (two cups or more daily). This habit might have no relevant connection with the QoL of the patient; nonetheless, a recent study on 335 hypertensive Chinese patients in Nanjing, China, suggested that selecting green tea or limiting tea consumption might reduce the risk of hyperhomocysteine in the hypertensive patients (Zhu et al., 2019). Another recent study reported that a higher consumption of green tea (> 3 cups/day) was inversely associated with stroke risk in middle-aged and older Korean men (Lee and Kim, 2019).
About 38.55% of the hypertensive patients indicated slight problems in the area of pain/discomfort and anxiety/depression. The highest percentage of a moderate problem (25.30%) and severe problem (9.64%) was found in the area of pain/discomfort (Table 1), which is similar to the previous studies (Bardage and Isacson, 2001; Zhang et al., 2017).
The patients participated in this study never had the time to do standard physical activity (3 times/week at 30 minutes). Most of these patients (72.3%) are unemployed or housewives with a comorbid disease (stroke). This study also proved that there is a significant relationship between physical exercise and the QoL of the patients.
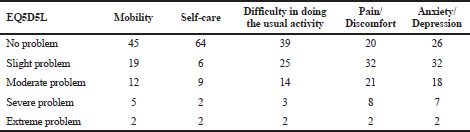 | Table 1. QoL measurements of the patients. [Click here to view] |
Physical activity was suggested to improve the wellness of the patients with stroke (Kim et al., 2016). Physical activity was reported to positively correlate with the adult HRQoL domains of 1,100 respondents in Brasov, Romania (Bădicu, 2018). Another study of Oza and coworkers concluded that the determinants of the QoL for the hypertensive patients were age, female gender, duration, number of symptoms, systolic blood pressure, and number of medication (Oza et al., 2014).
Table 2 shows that EQVAS score on exercise (p < 0.05) indicated a correlation between the patients’ exercise activity (defined by 30 minutes exercise 3 times/week) and the QoL of the patient. Moreover, Pearson correlation shows that the EQ5D5L score is positively related to EQVAS with a moderate degree of correlation (Sig. 0.469).
Of the 83 hypertensive participants, 37 patients (44.6%) were being treated with a single CCB, whereas 46 patients (55.4%) were being given the combination of CCB and ARB. Table 3 indicates that the best QoL (EQ5D5L score) was found in patients treated with a combination of nifedipine and candesartan (EQ5D5L score = 0.83 ± 0.04) which correlates with the patient’s self-health assessment (EQVAS score 0.75 + 0.06). Meanwhile, patients treated with a single CCB (either amlodipine EQ5D5L score = 0.51 ± 0.08 or nifedipine EQ5D5L score = 0.38 ± 0.53) indicated a lower score. Candesartan cilexetil is an angiotensin II type 1 receptor antagonist (ARB) that inhibits the actions of angiotensin II on the renin-angiotensin-aldosterone system. Oral candesartan of 8–32 mg once daily is recommended for the treatment of adult hypertensive patients (Cernes et al., 2011). A comparative study on the effect of candesartan versus telmisartan or valsartan had been carried out. 227 patients were grouped and treated with 40 mg telmisartan (n = 74), 8 mg candesartan cilexetil (n = 79), or 80 mg valsartan (n = 74) for 3 months. Results showed that both the systolic and diastolic blood pressures of all the groups significantly decreased at the end of the study; the decrease was comparable among the three groups (Ozaki et al., 2010).
Nonetheless, the presence of comorbidities in this study lowers the QoL of hypertensive patients. Some of the patients need a walking aid, particularly those who suffer from hemorrhagic stroke.
Comorbidities, e.g., stroke (Oza et al., 2014), Parkinson’s (Valkovic et al., 2015), epilepsy (Izci et al., 2016), end-stage renal disease (ESRD) (Lee et al., 2015), and osteoporosis (Barcenilla-Wong et al., 2015), which affected the QoL of the patients had been reported in other studies. The hypertensive patients with complicated illnesses resulted in a lower QoL were also reported (Zhang et al., 2017).
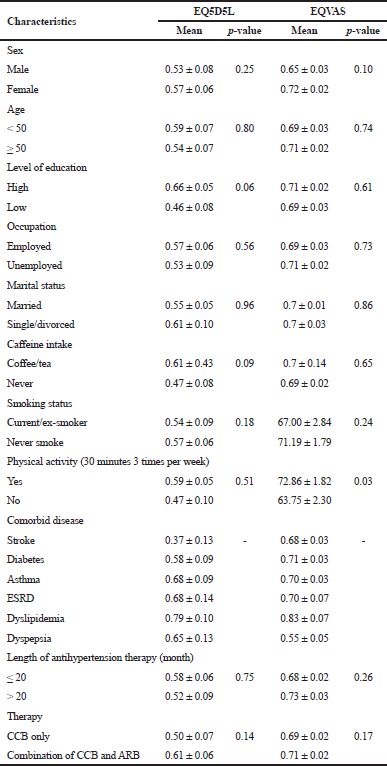 | Table 2. EQ5D5L and EQVAS score in the hypertensive patients. [Click here to view] |
This study has limitations. It included a small sample size (n = 83) due to the reluctance of most patients in participating in this project. Thus, certain variables could not be controlled.
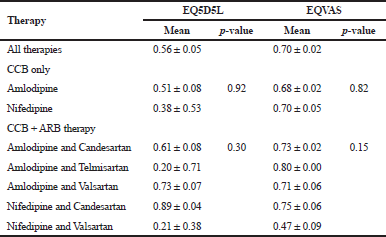 | Table 3. QoL scores based on hypertension therapy (P-value shows the relationship between variables with the QoL). [Click here to view] |