
INTRODUCTION
The World Health Organization (WHO) declared obesity a global epidemic (Jackson et al., 2020; Jayawardena et al., 2020). Overweight or obesity is a serious public health problem in Indonesia with a continuing increase in its prevalence (Rachmi et al., 2017). Based on the results of the Basic Health Research in Indonesia (2018), it is stated that the prevalence of obesity in adults has increased since the three Riskesdas periods, i.e., by 10.5% (2007), 14.8% (2013), and 21.8% (2018) (Damayanti et al., 2019). Obesity is caused by various factors including genetic, environmental, psychological, and health factors caused by the use of certain drugs and diseases, as well as factors in the development of adipose tissue (Fruh et al., 2017; Panuganti et al., 2021). However, the main cause of obesity is an imbalance between excessive food intake and low physical activity (Jehan et al., 2020; Romieu et al., 2017). Prevention of obesity can be achieved by changing lifestyle (Salam et al., 2020), such as increasing physical activity by exercising diligently and maintaining a healthy diet (Elliot and Hamlin, 2018; Koehler and Drenowatz, 2019).
High physical activity can be useful in the process of preventing obesity (Jakicic et al., 2019; Kim et al., 2017; Lorensia et al., 2021); on the other hand, low physical activity results in an increased prevalence of the risk of noncommunicable diseases such as heart disease, diabetes, and cancer (Ahmed et al., 2019; Saqib et al., 2020). Physical activity is defined as movement of the body by the muscles and skeleton which requires energy expenditure. There are two categories, namely moderate (moderate) and vigorous (strong) physical activity (Füzéki and Banzer, 2018; Hamer and Stamatakis, 2018). Both these types of physical activity provide health benefits and also affect vitamin D status (Skalska et al., 2019; Wici?ski et al., 2019). A person with vigorous and moderate activity has a higher vitamin D status than a person with low physical activity (Hall et al., 2018; Orces, 2019; Silva et al., 2019). Vitamin D status is also seen by dietary intake of foods containing vitamin D and daily lifestyle habits (Larson-Meyer et al., 2019; Suryadinata et al., 2020; Zadka et al., 2018), such as the use of sunscreen, low intake of milk (Aji et al., 2019), and avoiding sun exposure which causes a decrease in the synthesis of vitamin D by the skin resulting in vitamin D deficiency (Ramasamy, 2020; Suryadinata et al., 2020; Webb et al., 2018).
More than one billion people worldwide are deficient in vitamin D (Sizar et al., 2021). About 30%–50% of children and adults in the United Arab Emirates, Australia, Turkey, India, and Lebanon are deficient in vitamin D (Zarooni et al., 2019). The risk of vitamin D deficiency can occur in dark-skinned people, elderly patients, pregnant women, babies, people who do not get enough sun exposure, and obese individuals (Sizar et al., 2021; Suryadinata et al., 2021; Wacker and Holick, 2013). The body can get vitamin D by consuming milk, fish and fish oil, egg yolks, liver, and yeast (Maurya and Aggarwal, 2017; Polzonetti et al., 2020), exposure to sunlight, and taking vitamin D supplements (Kift et al., 2018; Lee et al., 2020). Vitamin D functions in the formation and maintenance of bones, so vitamin D deficiency results in bone abnormalities, namely rickets in children and osteomalacia in adults (Michigami, 2018; Takeuchi, 2018; Umar et al., 2018). Vitamin D deficiency also contributes to the development of cancer, especially breast, prostate, and colon cancer as well as heart disease, stroke, and autoimmune diseases (Charoenngam and Holick, 2020; Hassanalilou et al., 2017; Wang et al., 2017).
Early identification of vitamin D deficiency can be used as a preventive measure related to the risk of vitamin D deficiency (Aji et al., 2019; Pilz et al., 2019; Sizar et al., 2021). The indicators used to determine the status of vitamin D include blood tests, dietary food intake containing vitamin D (Aji et al., 2019; Lorensia et al., 2020a; Pilz et al., 2019), and questionnaires (Bolek-Berquist et al., 2009; Larson-Meyer et al., 2019). Evaluation of vitamin D status using a questionnaire is easier to carry out and more economical than blood serum examination. In addition, when compared to blood tests, clinical questionnaires can be used to identify long-term vitamin D status (Aji et al., 2019; Annweile et al., 2017; Bolek-Berquist et al., 2009). The questionnaire can be used to identify patients who are at high or low risk of experiencing vitamin D deficiency (Bolek-Berquist et al., 2009). Obesity as a risk factor for vitamin D deficiency (Paschou et al., 2019) needs to get prevention efforts as early as possible considering the dangers of vitamin D deficiency and low physical activity as causes of obesity which affect the development of chronic diseases and decreased quality of life (Kavadar et al., 2015; Kim et al., 2018; Oh et al., 2017).
This study involved young adult respondents because adults were of productive age and relatively had high physical activity. However, nowadays, there are many young adults who actually experience vitamin D deficiency and rarely do physical activity (Lorensia et al., 2019). This research was conducted on university students because education can affect a person’s physical activity and lifestyle (Kotarska et al., 2021). It was, therefore, necessary to identify vitamin D status and physical activity in obese and nonobese adults so that pharmacists can provide education to the public, both obese and nonobese adults, as a form of health workers’ responsibility in early prevention efforts related to the risk of deficiency of vitamin D and other health problems.
METHODS
Research design
The design of this study was cross-sectional and was conducted on a group of students with nonobese and obese nutritional status in the campus area of the University of Surabaya. The research location chosen to conduct the research was the campus area in South Surabaya, Rungkut district, East Java, Indonesia, and the study was carried out from March 2018 to January 2019. This study was approved with Ethical Test No. 034/KE/I/2018 at Universitas Surabaya.
Research variable
The independent variable in this study was a group of obese and nonobese respondents. The dependent variables in this study were vitamin D status and physical activity. Vitamin D status can be defined as the presence of vitamin D in a certain amount in the body which was influenced by the intake of foods containing vitamin D, sun exposure, and consumption of vitamin D supplements. A person was said to be positive (+) (at risk) of vitamin D deficiency if the total answer score was ≥15 and negative (−) if the total answer score was <15. Vitamin D deficiency is a health problem related to vitamin D status. The risk of vitamin D deficiency in nonobese and obese respondents is calculated using the prevalence odds ratio equation.
Physical activity was defined as body movement by the muscles and skeleton which requires energy expenditure, including activities carried out while working, playing, doing household chores, traveling, and recreation. Physical activity in adults can be measured using the International Physical Activity Questionnaire (IPAQ) (Cleland et al., 2018; Kavadar et al., 2015; Sember et al., 2020). This can be measured by asking seven questions related to daily activities. The data scale obtained from the measurement of physical activity was an ordinal data scale, where the results obtained from the patient questionnaire were categorized into low, medium, and high physical activity (Table 1).
Obesity was characterized by the accumulation of excess body fat tissue (De Lorenzo et al., 2019). Determination of obesity status in individuals was based on the measurement of body mass index (BMI), a person's body weight (in kg) divided by the square of height (in m). The International Association for Study of Obesity Organization, International Obesity Task Force, and WHO determined the category of obesity for the Asian population if the BMI was ≥25 kg/m2. Therefore, in this study, BMI points ≥25 kg/m2 were used to determine the obesity category.
Population and sample
The population used in this study was all students at the University of Surabaya with a nutritional status of obesity or nonobesity. The sample used in this study was active students at the University of Surabaya with a nutritional status conditions of obesity or nonobesity who met the criteria, including 18–25-year-olds, those with no special diet (such as fasting or vegetarianism), those who did not have certain diseases like cardiovascular disorders such as angina, renal, and hepatic disorders (such as cirrhosis of the liver), and individuals who have no motoric problems. The sampling technique used was the purposive sampling method, in which the sampling process was based on previously known characteristics or characteristics of the population and the consideration of the researcher.
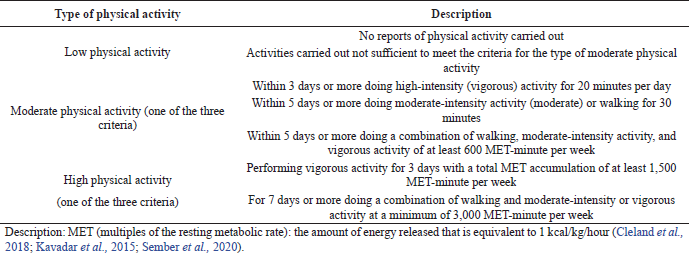 | Table 1. Guidelines for assessment of physical activity based on the IPAQ. [Click here to view] |
Data collection methods and analysis
Measuring instruments used in the study were the vitamin D status questionnaire to identify vitamin D status and the IPAQ for physical activity data. Measurements of weight and height were carried out using a digital weight scale and a Microtoise stature meter, respectively. There were two types of questionnaires given, namely the vitamin D status questionnaire (Bolek-Berquist et al., 2009; Cairncross et al., 2017; Nabak et al., 2014) and the IPAQ (Cleland et al., 2018; Kavadar et al., 2015; Sember et al., 2020).
We conducted a trial or pilot study where data collection was preceded by testing the research instruments on 30 respondents. The questionnaire was validated using internal and external validity methods. Internal validity was enforced in a review step based on professional opinion judgments in the field of community pharmacy, while external validation was carried out by testing the questionnaire on the subject. Then, the results were analyzed using the Statistical Package for the Social Sciences (SPSS) version 24.0 computer program. The questionnaire was said to be valid if the value of rcount > 0.361. The questionnaire was rehabilitated using a single trial method technique with the alpha method (Cronbach), namely testing the reliability of the questionnaire once on respondents who have criteria such as research subjects, but these subjects are not used as samples. A reliability test can be carried out on valid questions. The calculation of the reliability coefficient uses the SPSS version 24.0 software. The questionnaire was declared reliable if the Cronbach’s alpha value was >0.70.
Comparative analysis of the risk of vitamin D deficiency was based on vitamin D status in the obese and nonobese groups of respondents using the prevalence odds ratio. Meanwhile, differences in vitamin D status and physical activity in the obese and nonobese respondent groups used the chi-square test. We then proceeded to test the relationship between vitamin D status and physical activity in the groups of obese and nonobese respondents using a contingency coefficient.
RESULTS
The data obtained in this study were obtained through a vitamin D status questionnaire and the IPAQ. The data collection process uses instruments that are valid and reliable. Based on the data obtained, there were 143 respondents consisting of 2 groups, namely the obese group consisting of 71 people (49.65%) and the nonobese group consisting of 72 people (50.34%).
Validity and reliability of the IPAQ
The original IPAQ was available in English. The validation process was carried out by translating the questionnaire into Indonesian and then giving it to three professional judges in the field of community pharmacy. The validity was enforced in the analysis step based on the opinion of professional judges in the field of community pharmacy.
Validity and reliability of the vitamin D status questionnaire
The reliability of the questionnaire was determined based on Cronbach’s alpha value. The questionnaire was declared reliable if Cronbach’s alpha value was >0.60. The Cronbach’s alpha value of the vitamin D status questionnaire was 0.735, so the questionnaire was declared reliable. The questionnaire validation process used the SPSS version 24.0 program. The validation process was carried out on 30 respondents. Based on the Pearson product–moment rtable with a significance of 0.05 with a two-sided test and the amount of data (n) = 30, it was known that rtable value was 0.361 so that rcount > 0.361, and it can be concluded that the questionnaire was valid.
Respondent characteristics
In this study, the respondents included were students with a stratum 1 education level with an age range of 18–25 years. Table 2 explains the distribution of respondents’ age, sex, and BMI.
The results of the answers to the two groups of respondents were classified into sections regarding sun exposure (Table 3), foods containing vitamin D (Table 4), and signs of vitamin D deficiency (Table 5).
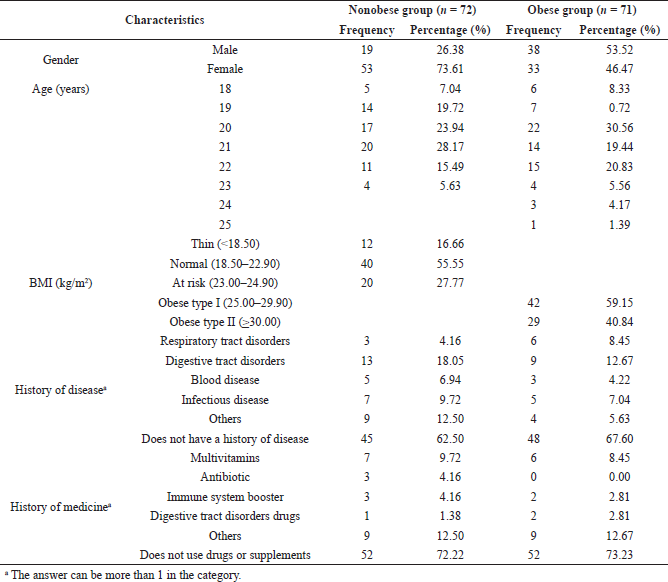 | Table 2. Characteristics of respondents. [Click here to view] |
The nonobese group had a more positive vitamin D status (≥15) (76.39%) than the obese group. At the same time, the level of activity in the nonobese group was dominated by moderate (55.55%) compared to the obese group, which was dominated by low activity levels (61.97%) (Table 6).
Based on the results of the analysis with the chi-square test to see the difference in vitamin D status between the nonobese and obese respondent groups, it was found that there was a significant difference (p-value <0.05) in the vitamin D status of the nonobese and obese groups of respondents (Table 7).
Based on the results of the analysis with the chi-square test to see the difference in physical activity between the groups of nonobese and obese respondents, it was shown that there was significant difference between the two (p-value <0.05) (Table 8).
Based on the contingency coefficient correlation test for vitamin D status and physical activity in the nonobese and obese respondent groups, the approximate significance value of 0.000 (p = 0.000) indicated that there was a significant relationship between vitamin D status and physical activity and the relationship has a correlation value of 0.326, so it can be concluded that there is a significant relationship between physical activity and vitamin D status in the nonobese and obese respondent groups, but the relationship was low or weak (Table 9).
DISCUSSION
Respondents who were involved in this study were 143 people and consisted of male sex at 39.86% (57 people) and female sex at 60.13% (86 people). The group of respondents in the category of male obesity were as many as 53.52% (38 people) and female sex as many as 46.47% (33 people) and for respondents with nonobesity categories, male respondents as many as 26.38% (19 people) and women 73.61% (53 people). Gender can affect vitamin D status; the female sex has a low vitamin status compared to the male sex (Annweiler et al., 2017; AlQuaiz et al., 2018; Sanghera et al., 2017) due to avoiding sun exposure and dress habits are one of the main factors (Kift et al., 2018; Lee and Lee, 2020) such as wearing long-sleeved shirts, long skirts, and headscarves (Judistiani et al., 2019; Pulungan et al., 2021). Gender not only affects vitamin D status but also affects physical activity (Fernandes and Junior, 2017; Wici?ski et al., 2019). History of disease and use of drugs have a relationship with vitamin D status in the body. Certain pathological conditions, such as Crohn’s disease, cystic fibrosis, celiac disease, and surgical removal of parts of the stomach or intestines that play a role in fat absorption, can trigger vitamin D deficiency. Anticonvulsant drugs are also called antiepileptic drugs. The long duration of some antiepileptic drugs, such as phenobarbital, phenytoin, and carbamazepine, and the antimicrobial agent rifampin can cause osteomalacia, which is a condition caused by vitamin D deficiency. This is triggered by the induction of 1,25-dihydroxyvitamin D catabolism (Saket et al., 2021). Men tend to be more active than women, because spend more time sitting and doing activities that smell of cosmetic, Women tend to be inactive compared to men. Women spend more time sitting and doing activities that smell of cosmetic while the male sex prefers to do sports so the activities carried out are higher than women (Sharifi et al., 2016).
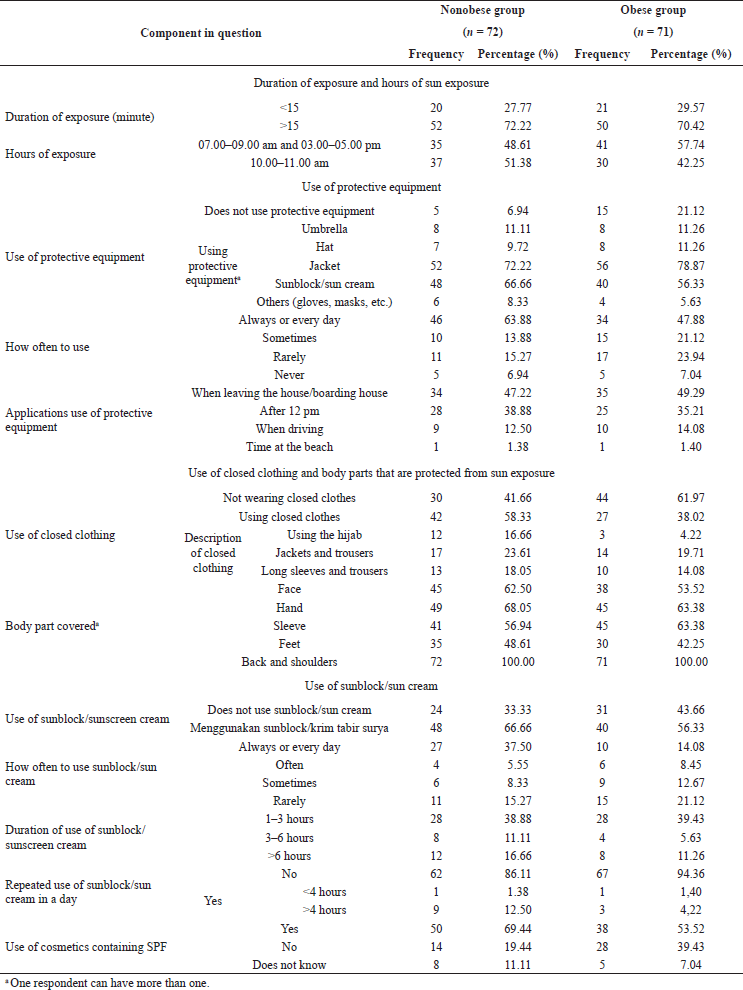 | Table 3. Distribution of respondents’ answers regarding length of exposure and hours of sun exposure. [Click here to view] |
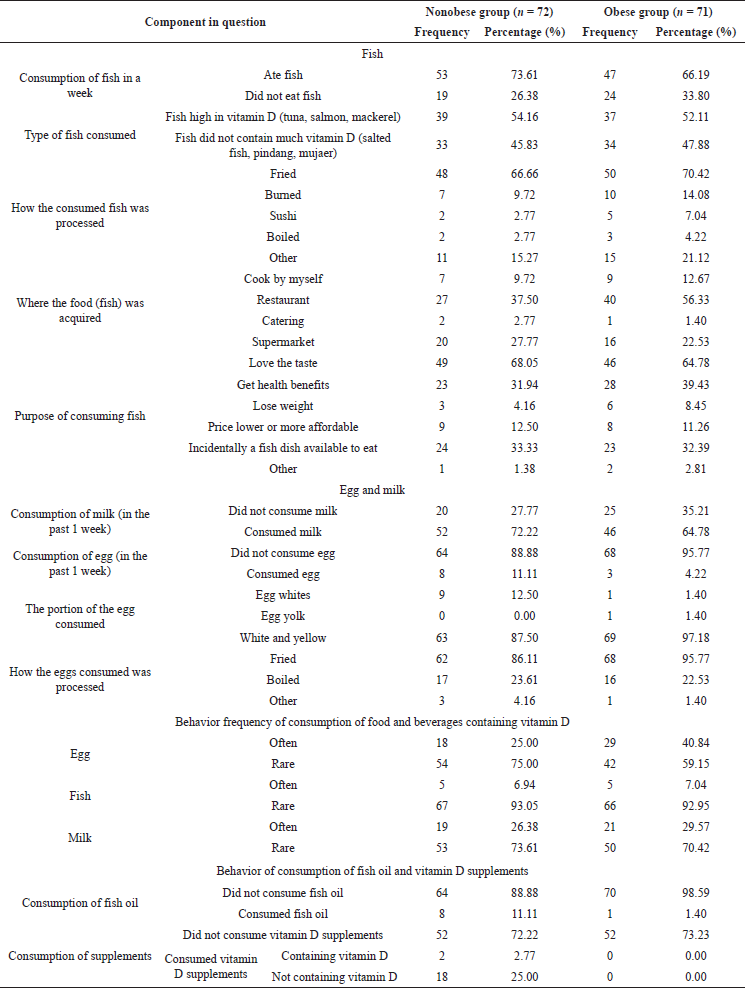 | Table 4. Distribution of respondents’ answers regarding foods containing vitamin D. [Click here to view] |
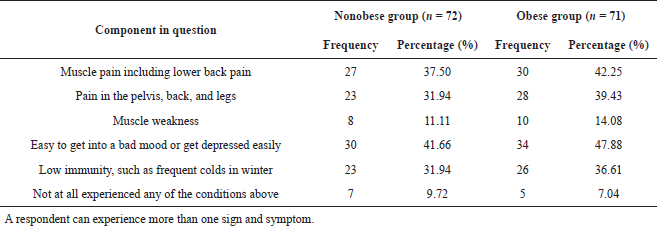 | Table 5. Distribution of respondents’ answers regarding signs of vitamin D deficiency. [Click here to view] |
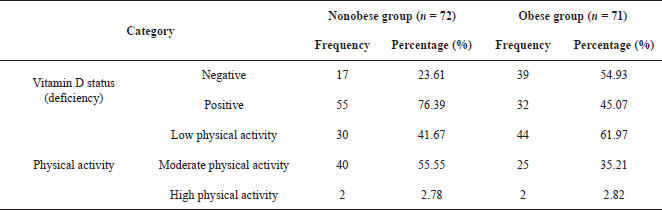 | Table 6. Cross-tabulation of vitamin D status and physical activity in the nonobese and obese respondents. [Click here to view] |
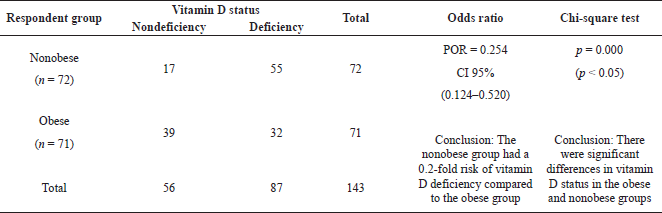 | Table 7. Risk analysis and differences test of vitamin D deficiency related to vitamin D status in nonobese and obese respondents. [Click here to view] |
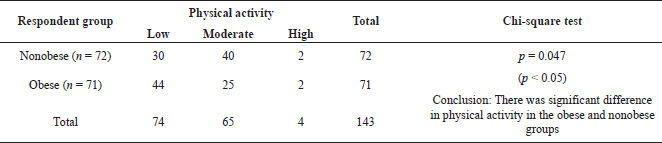 | Table 8. Risk analysis and differences test in physical activity in nonobese and obese respondents. [Click here to view] |
 | Table 9. Results of analysis of the relationship between vitamin D status and physical activity. [Click here to view] |
All respondents involved in this study were aged 18–25 years and were active students. This study uses young adult respondents because based on previous research young adults are known to be at risk of vitamin D deficiency which is influenced by habits such as consumption of vitamin D below the recommended limit per day, lack of outdoor physical activity, increased use of sunblock/sunscreen cream, and low milk intake (Bolek-Berquist et al., 2009). In addition to young adults, the elderly are also one of the age groups that have a low risk of vitamin D status. Low vitamin D status can cause muscle weakness (Gunton and Girgis, 2018; Sizar et al., 2021) and increase the risk of fractures in the elderly (Thanapluetiwong et al., 2020).
Obesity is a risk factor for vitamin D deficiency (Paschou et al., 2019) based on the research by Kavadar et al., (2015) that found a relationship between obesity and low vitamin D status, which has an impact on the risk of insulin resistance. The mechanism of vitamin D deficiency in obese patients is not precisely known, but several researchers have hypothesized that, related to the mechanism of vitamin D deficiency in obese patients, high fat accumulation results in a decrease in vitamin D bioavailability, where a lot of vitamin D is stored in fat cells in adipose tissue and increases vitamin D deficiency. Oxidative reactions, due to the fat-soluble nature of vitamin D, cause a decrease in the release of vitamin D from fat into the systemic circulation (Wimalawansa, 2019) in obese patients. One of the causes of obesity is excessive food intake, low physical activity (Romieu et al., 2017), and lack of rest hours; besides that, there is a relationship between age and workplace characteristics on the risk of becoming obese (Hruby et al., 2016). Low physical activity is found in obese people (Kim et al., 2017); therefore, increasing physical activity can be used as an appropriate step to prevent the risk of obesity and weight loss (Jakicic et al., 2019).
Long exposure can affect the synthesis of vitamin D by the body; an exposure time of 15 minutes can synthesize vitamin D of 10,000–25,000 IU over a large area of the body surface and is characterized by a change in skin color to pink (Suryadinata et al., 2021). In this study, the results showed that, in the two groups of respondents who were obese and nonobese, those who received longer sun exposure (>15 minutes) were the nonobese group of 36.36% (52 people) compared to the obese group of 36.36% (52 people). The most dominant group with less exposure to sunlight (<15 minutes) was the obese group at as much as 14.68% (21 people) and then the nonobese group at 13.98% (20 people). One of the factors that influence the duration of exposure to vitamin D synthesis is skin type (Wacker and Holick, 2013). Different skin types affect the length of time it takes the skin to synthesize vitamin D. Dark skin type (type IV skin) requires a long exposure time of six times longer than skin type I (Wacker and Holick, 2013). This is influenced by the pigment in the skin called melanin which functions as a natural sunscreen that can block the absorption of sunlight by the skin (Solano, 2020). Asian skin is in skin type IV or V; therefore, Asian people need a longer exposure time than other skin types. The recommended exposure time is more than 15 minutes or even up to 2 hours (Webb et al., 2018). Exposure time is also an important factor in the process of vitamin D synthesis (Suryadinata et al., 2021). It is known from the results of this study that the highest Ultraviolet B (UVB) intensity occurs from 11.00 am to 01.00 pm (Lorensia et al., 2020b). UVB rays obtained from sunlight can help the synthesis of vitamin D in the skin (Wacker et al., 2013; Lee and Lee, 2020).
One source of vitamin D is fish. The highest amount of vitamin D is found in fish liver (2–477 mg/kg), a maximum of 1,200 mg/kg and depending on the type of fish (Schmid and Walther, 2013). A total of 66.19% (47 people) of the obese respondent group, who consumed fish within the past week, consumed fish with vitamin D content of 52.11% (37 people), while in the nonobese respondent group of a total of 73.61% (53 people) who consumed fish as many as 54.16% (39 people) consumed fish with vitamin D content. The obese respondent group (7.04%) and the nonobese respondent group (6.94%) often consumed fish in the last week The frequency of fish consumption can affect vitamin D status. In Japan, fish is the main source for obtaining vitamin D (Nakamura et al., 2002). The cooking process does not really affect the vitamin D content in food products because vitamin D is resistant to heat (Schmid and Walther, 2013), but the fish processing process also affects the amount of vitamin D.
Eggs are a source of vitamin D (Schmid and Walther, 2013). The obese respondents who consumed eggs were 95.77% (68 people), and the nonobese respondents who consumed eggs were 88.88% (64 people). The respondents from the obese group who often consumed eggs within 1 week were 40.84% (29 people), and the respondents from the nonobese group were 25% (18 people). Vitamin D in eggs is found in the yolk at as much as 20 IU of vitamin D3 or D2 per egg yolk (Schmid and Walther, 2013). In addition to eggs and fish, milk is also a fortification product that contains vitamin D (Lorensia et al., 2020b; Schmid and Walther, 2013). Someone with low milk consumption can experience vitamin D deficiency (Bolek-Berquist et al., 2009).
Based on the results of the analysis with the chi-square test, the p-value of 0.047 (p-value <0.05) can be concluded so it can be concluded that there is a significant difference in physical activity between the nonobese and obese groups of respondents. This is supported by evidence from previous studies which showed that there was a significant difference in physical activity in the normal group compared to the obese group, where the obese group had a longer sitting time than the nonobese group, and obesity had a significant relationship with low physical activity and physical function (Hong et al., 2016).
In the analysis of the relationship between vitamin D status and physical activity using the contingency coefficient correlation test, we obtained an approximate significance value of 0.000 (p-value = 0.000), which indicates that there is a significant relationship between vitamin D status and physical activity and the relationship has a correlation value of 0.326. Based on the contingency coefficient table, the two variables have a low or weak relationship but are definitely related so it can be concluded that there is a relationship between vitamin D status and physical activity in the nonobese and obese respondent groups, but the relationship is low or weak. This is in accordance with previous research which showed that a person with low physical activity has a low vitamin D status (Aji et al., 2019). In addition, high outdoor physical activity can increase vitamin D status (Lorensia et al., 2021). Outdoor physical activity, which is in exposure to sunlight, is statistically significant in increasing vitamin D status (Lorensia et al., 2020a). Therefore, physical activity and dietary intake of vitamin D should be increased in an effort to prevent vitamin D deficiency and other health problems such as metabolic risk factors (Lorensia et al., 2020a). There are some limitations in this research, including the existence of variables that can affect the results of the study such as the uneven distribution of sexes between the two groups of respondents being compared, and there is no examination of serum 25(OH)D for determining vitamin D levels.
CONCLUSION
There is a significant difference in vitamin D status in the obese and nonobese groups of respondents, and there is a significant difference in physical activity in the obese and nonobese groups of respondents. In addition, there is a significant relationship between vitamin D status and physical activity, but the relationship between the two is low or weak.
ACKNOWLEDGMENT
This research was funded by the Institute of Research and Community Service by Universitas Surabaya.
CONFLICTS OF INTEREST
The authors declare no conflicts of interest.
DATA AVAILABILITY
All data generated and analyzed are included within this research article.
PUBLISHER’S NOTE
This journal remains neutral with regard to jurisdictional claims in published institutional affiliation.
REFERENCES
Ahmed SH, Meyer HE, Kjøllesdal MK, Marjerrison N, Mdala I, Htet AS, Bjertness E, Madar AA. The prevalence of selected risk factors for non-communicable diseases in Hargeisa, Somaliland: a cross-sectional study. BMC Public Health, 2019; 19(1):878. CrossRef
Aji AS, Erwinda E, Yusrawati Y, Malik SG, Lipoeto NI. Vitamin D deficiency status and its related risk factors during early pregnancy: a cross-sectional study of pregnant Minangkabau women, Indonesia. BMC Pregnancy Childbirth, 2019; 19(1):183. CrossRef
AlQuaiz AM, Kazi A, Fouda M, Alyousefi N. Age and gender differences in the prevalence and correlates of vitamin D deficiency. Arch Osteoporos, 2018; 13(1):49. CrossRef
Annweiler C, Kabeshova A, Callens A, Paty ML, Duval GT, Holick MF. Self-administered vitamin D status predictor: older adults are able to use a self-questionnaire for evaluating their vitamin D status. PLoS One, 2017; 12(11):e0186578. CrossRef
Bolek-Berquist J, Elliott ME, Gangnon RE, Gemar D, Engelke J, Lawrence SJ, Hansen KE. Use of a questionnaire to assess vitamin D status in young adults. Public Health Nutr, 2009; 12(2):236–43. CrossRef
Cairncross CT, Stonehouse W, Conlon CA, Grant CC, McDonald B, Houghton LA, Eyles D, Camargo CA Jr, Coad J, von Hurst PR. Predictors of vitamin D status in New Zealand preschool children. Matern Child Nutr, 2017; 13(3):e12340. CrossRef
Charoenngam N, Holick MF. Immunologic effects of vitamin D on human health and disease. Nutrients, 2020; 12(7):2097. CrossRef
Cleland C, Ferguson S, Ellis G, Hunter RF. Validity of the International Physical Activity Questionnaire (IPAQ) for assessing moderate-to-vigorous physical activity and sedentary behaviour of older adults in the United Kingdom. BMC Med Res Methodol, 2018; 18(1):176. CrossRef
Damayanti RA, Sumarmi S, Mundiastuti L. The association between sleep duration with overweight and obesity among education staff in campus C of Universitas Airlangga. Amerta Nutr, 2019; 3(2):89–93. CrossRef
De Lorenzo A, Gratteri S, Gualtieri P, Cammarano A, Bertucci P, Di Renzo L. Why primary obesity is a disease? J Transl Med, 2019; 17(1):169. CrossRef
Elliot CA, Hamlin MJ. Combined diet and physical activity is better than diet or physical activity alone at improving health outcomes for patients in New Zealand's primary care intervention. BMC Public Health, 2018; 18(1):230. CrossRef
Fernandes MR, Junior DRBJ. Association between physical activity and vitamin D: a narrative literature review. Rev Assoc Med Bras, 2017; 63(6):550–6. CrossRef
Fruh SM. Obesity: risk factors, complications, and strategies for sustainable long-term weight management. J Am Assoc Nurse Pract, 2017; 29(S1):S3–14. CrossRef
Füzéki E, Banzer W. Physical activity recommendations for health and beyond in currently inactive populations. Int J Environ Res Public Health, 2018; 15(5):1042. CrossRef
Gunton JE, Girgis CM. Vitamin D and muscle. Bone Rep, 2018; 8:163–7. CrossRef
Hall JT, Ebeling M, Shary JR, Forestieri N, Wagner CL. The relationship between physical activity and vitamin D status in postpartum lactating and formula-feeding women. J Steroid Biochem Mol Biol, 2018; 177:261–5. CrossRef
Hamer M, Stamatakis E. Relative proportion of vigorous physical activity, total volume of moderate to vigorous activity, and body mass index in youth: the Millennium Cohort Study. Int J Obes, 2018; 42(6):1239–42. CrossRef
Hassanalilou T, Khalili L, Ghavamzadeh S, Shokri A, Payahoo L, Bishak YK. Role of vitamin D deficiency in systemic lupus erythematosus incidence and aggravation. Auto Immun Highlights, 2017; 9(1):1. CrossRef
Hong I, Coker-Bolt P, Anderson KR, Lee D, Velozo CA. Relationship between physical activity and overweight and obesity in children: findings from the 2012 National Health and Nutrition Examination Survey National Youth Fitness Survey. Am J Occup Ther, 2016; 70(5):7005180060p1–8. CrossRef
Hruby A, Manson JE, Qi L, Malik VS, Rimm EB, Sun Q, Willett WC, Hu FB. Determinants and consequences of obesity. Am J Public Health, 2016; 106(9):1656–62. CrossRef
Jackson SE, Llewellyn CH, Smith L. The obesity epidemic—nature via nurture: a narrative review of high-income countries. SAGE Open Med, 2020; 8:2050312120918265. CrossRef
Jakicic JM, Powell KE, Campbell WW, Dipietro L, Rate RR, Pescatello LS, Collins KA, Bloodgood B, Piercy KL. Physical activity and the prevention of weight gain in adults: a systematic review. Med Sci Sports Exerc, 2019; 51(6):1262–9. CrossRef
Jayawardena R, Jeyakumar DT, Misra A, Hills AP, Ranasinghe P. Obesity: a potential risk factor for infection and mortality in the current COVID-19 epidemic. Diabetes Metab Syndr, 2020; 14(6):2199–203. CrossRef
Jehan S, Zizi F, Pandi-Perumal SR, McFarlane SI, Jean-Louis G, Myers AK. Energy imbalance: obesity, associated comorbidities, prevention, management and public health implications. Adv Obes Weight Manag Control, 2020; 10(5):146–61. CrossRef
Judistiani RTD, Nirmala SA, Rahmawati M, Ghrahani R, Natalia YA, Sugianli AK, Indrati AR, Suwarsa O, Setiabudiawan B. Optimizing ultraviolet B radiation exposure to prevent vitamin D deficiency among pregnant women in the tropical zone: report from cohort study on vitamin D status and its impact during pregnancy in Indonesia. BMC Pregnancy Childbirth, 2019; 19(1):209. CrossRef
Kavadar G, Demircio?lu DT, Özgönenel L, Emre TY. The relationship between vitamin D status, physical activity and insulin resistance in overweight and obese subjects. Bosn J Basic Med Sci, 2015; 15(2):62–6. CrossRef
Kift R, Rhodes LE, Farrar MD, Webb AR. Is sunlight exposure enough to avoid wintertime vitamin d deficiency in United Kingdom population groups? Int J Environ Res Public Health, 2018; 15(8):1624. CrossRef
Kim BY, Choi DH, Jung CH, Kang SK, Mok JO, Kim CH. Obesity and physical activity. J Obes Metab Syndr, 2017; 26(1):15–22. CrossRef
Kim SH, Oh JE, Song DW, Cho CY, Hong SH, Cho YJ, Yoo BW, Shin KS, Joe H, Shin HS, Son DY. The factors associated with vitamin D deficiency in community dwelling elderly in Korea. Nutr Res Pract, 2018; 12(5):387–95. CrossRef
Koehler K, Drenowatz C. Integrated role of nutrition and physical activity for lifelong health. Nutrients, 2019; 11(7):1437. CrossRef
Kotarska K, Nowak MA, Nowak L, Król P, Sochacki A, Sygit K, Sygit M. Physical activity and quality of life of university students, their parents, and grandparents in poland-selected determinants. Int J Environ Res Public Health, 2021; 18(8):3871. CrossRef
Larson-Meyer DE, Douglas CS, Thomas JJ, Johnson EC, Barcal JN, Heller JE, Hollis BW, Halliday TM. Validation of a vitamin D specific questionnaire to determine vitamin D status in athletes. Nutrients, 2019; 11(11):2732. CrossRef
Lee YM, Kim SA, Lee DH. Can current recommendations on sun exposure sufficiently increase serum vitamin d level? One-month randomized clinical trial. J Korean Med Sci, 2020; 35(8):e50. CrossRef
Lorensia A, Suryadinata RV, Saputra R. Physical activity and vitamin D level in asthma and non-asthma. J Farmasi Indones, 2019; 11(1):454–65.
Lorensia A, Muntu CM, Suryadinata RV, Septiani R. Effect of lung function disorders and physical activity on smoking and non-smoking students. J Prev Med Hyg, 2021; 62(1):E89–96. CrossRef
Lorensia A, Wahyudi M, Yudiarso A, Kurnia SED. Effect of illness perception on improving asthma symptoms with omega-3 fish oil therapy: Pre-post design. J Appl Pharm Sci, 2020a; 10(6):62–71. CrossRef
Lorensia A, Suryadinata RV, Chandra NLMR. Profile of vitamin D status, physical activity, and lung health in construction workers (profil status vitamin D, Aktivitas Fisik, dan Kesehatan Paru pada Tukang Bangunan). Community Med Public Health Indones J, 2020b; 1(2):117–24. CrossRef
Maurya VK, Aggarwal M. Factors influencing the absorption of vitamin D in GIT: an overview. J Food Sci Technol, 2017; 54(12):3753–65.
Michigami T. Rickets/osteomalacia. Consensus on Vitamin D deficiency and insufficiency in children. Clin Calcium Jpn, 2018; 28(10):1307–11. CrossRef
Nabak A, Johnson R, Keuler N, Hansen K. Can a questionnaire predict vitamin D status in postmenopausal women? Public Health Nutr, 2014; 17(4):739–46. CrossRef
Nakamura K, Nashimoto M, Okuda Y, Ota T, Yamamoto M. Fish as a major source of vitamin D in the Japanese diet. Nutrition, 2002; 18(5):415–6. CrossRef
Oh TR, Kim CS, Bae EH, Ma SK, Han SH, Sung SA, Lee K, Oh KH, Ahn C, Kim SW. Association between vitamin D deficiency and health-related quality of life in patients with chronic kidney disease from the KNOW-CKD study. PLoS One, 2017; 12(4):e0174282. CrossRef
Orces C. The association between body mass index and vitamin D supplement use among adults in the United States. Cureus, 2019; 11(9):e5721.
Panuganti KK, Nguyen M, Kshirsagar RK. Obesity. StatPearls, Treasure Island, FL, 2021. [ONLINE] Available via https://www.ncbi.nlm.nih.gov/books/NBK459357/ (Accessed 11 August 2021). CrossRef
Paschou SA, Kosmopoulos M, Nikas IP, Spartalis M, Kassi E, Goulis DG, Lambrinoudaki I, Siasos G. The impact of obesity on the association between vitamin D deficiency and cardiovascular disease. Nutrients, 2019; 11(10):2458. CrossRef
Pilz S, Zittermann A, Trummer C, Theiler-Schwetz V, Lerchbaum E, Keppel MH, Grubler MR, Marz W, Pandis M. Vitamin D testing and treatment: a narrative review of current evidence. Endocr Connect, 2019; 8(2):R27–43. CrossRef
Polzonetti V, Pucciarelli S, Vincenzetti S, Polidori P. Dietary Intake of Vitamin D from dairy products reduces the risk of osteoporosis. Nutrients, 2020; 12(6):1743. CrossRef
Pulungan A, Soesanti F, Tridjaja B, Batubara J. Vitamin D insufficiency and its contributing factors in primary school-aged children in Indonesia, a sun-rich country. Ann Pediatr Endocrinol Metab, 2021; 26(2):92–8. CrossRef
Rachmi CN, Li M, Alison Baur L. Overweight and obesity in Indonesia: prevalence and risk factors-a literature review. Public Health, 2017; 147:20–9. CrossRef
Ramasamy I. Vitamin D metabolism and guidelines for vitamin D supplementation. Clin Biochem Rev, 2020; 41(3):103–26. CrossRef
Romieu I, Dossus L, Barquera S, Blottiere HM, Franks PW, Gunter M, Hwalla N, Hursting SD, Leitzmann M, Margetts B, Nishida C. Energy balance and obesity: what are the main drivers? Cancer Causes Control, 2017; 28(3):247–58.
Saket S, Varasteh N, Halimi Asl AA, Saneifard H. How antiepileptics may change the serum level of vitamin D, calcium, and phosphorus in children with epilepsy. Iran J Child Neurol, 2021; 15(1):19–27.
Salam RA, Padhani ZA, Das JK, Shaikh AY, Hoodbhoy Z, Jeelani SM, Lassi ZS, Bhutta ZA. Effects of lifestyle modification interventions to prevent and manage child and adolescent obesity: a systematic review and meta-analysis. Nutrients, 2020; 12(8):2208. CrossRef
Sanghera DK, Sapkota BR, Aston CE, Blackett PR. Vitamin D status, gender differences, and cardiometabolic health disparities. Ann Nutr Metab, 2017; 70(2):79–87. CrossRef
Saqib ZA, Dai J, Menhas R, Mahmood S, Karim M, Sang X, Weng Y. Physical activity is a medicine for non-communicable diseases: a survey study regarding the perception of physical activity impact on health wellbeing. Risk Manag Healthc Policy, 2020; 13:2949–62. CrossRef
Schmid A, Walther B. Natural vitamin D content in animal products. Adv Nutr, 2013; 4(4):453–62. CrossRef
Sember V, Meh K, Sori? M, Starc G, Rocha P, Jurak G. Validity and reliability of international physical activity questionnaires for adults across EU countries: systematic review and meta-analysis. Int J Environ Res Public Health, 2020; 17(19):7161. CrossRef
Sharifi N, Amani R, Hajiani E, Cheraghian B. Women may respond different from men to vitamin D supplementation regarding cardiometabolic biomarkers. Exp Biol Med (Maywood), 2016; 241(8):830–8. CrossRef
Silva ACMD, Cureau FV, de Oliveira CL, Giannini DT, Bloch KV, Kuschnir MCC, Dutra ES, Schaan BD, de Carvalho KMB. Physical activity but not sedentary time is associated with vitamin D status in adolescents: study of cardiovascular risk in adolescents (ERICA). Eur J Clin Nutr, 2019; 73(3):432–40. CrossRef
Sizar O, Khare S, Goyal A, Givler A. Vitamin D deficiency. StatPearls, Treasure Island, FL, 2021. [ONLINE] Available via https://www.ncbi.nlm.nih.gov/books/NBK532266/ (Accessed 12 April 2021).
Skalska M, Nikolaidis PT, Knechtle B, Rosemann TJ, Radziminski L, Jastrzebska J, Kaczmarczyk M, My?liwiec A, Dragos P, López-Sánchez GF, Jastrz?bski Z. Vitamin D supplementation and physical activity of young soccer players during high-intensity training. Nutrients, 2019; 11(2):349. CrossRef
Solano F. Photoprotection and skin pigmentation: melanin-related molecules and some other new agents obtained from natural sources. Molecules, 2020; 25(7):1537. CrossRef
Suryadinata RV, Boengas S, Lorensia A. Effect of knowledge and attitude toward sun exposure related vitamin D to lung function. Teikyo Med J, 2021; 44(4):957–69.
Suryadinata RV, Wirjatmadi B, Andriani M, Lorensia A. Effect of age and weight on physical activity. J Publich Health Res, 2020; 9(2):187–90. CrossRef
Takeuchi Y. Rickets/osteomalacia. Treatment of vitamin D deficiency in adults. Clin Calcium, 2018; 28(10):1387–92.
Thanapluetiwong S, Chewcharat A, Takkavatakarn K, Praditpornsilpa K, Eiam-Ong S, Susantitaphong P. Vitamin D supplement on prevention of fall and fracture: a meta-analysis of randomized controlled trials. Medicine (Baltimore), 2020; 99(34):e21506. CrossRef
Umar M, Sastry KS, Chouchane AI. Role of vitamin D beyond the skeletal function: a review of the molecular and clinical studies. Int J Mol Sci, 2018; 19(6):1618. CrossRef
Wacker M, Holick MF. Sunlight and vitamin D: a global perspective for health. Dermatoendocrinol, 2013; 5(1):51–108. CrossRef
Wang H, Chen W, Li D, Yin X, Zhang X, Olsen N, Zheng SG. Vitamin D and chronic diseases. Aging Dis, 2017; 8(3):346–53. CrossRef
Webb AR, Kazantzidis A, Kift RC, Farrar MD, Wilkinson J, Rhodes LE. Colour counts: sunlight and skin type as drivers of vitamin D deficiency at UK Latitudes. Nutrients, 2018; 10(4):457. CrossRef
Wici?ski M, Adamkiewicz D, Adamkiewicz M, ?niegocki M, Podhorecka M, Szychta P, Malinowski B. Impact of vitamin D on physical efficiency and exercise performance-a review. Nutrients, 2019; 11(11):2826. CrossRef
Wimalawansa SJ. Vitamin D deficiency: effects on oxidative stress, epigenetics, gene regulation, and aging. Biology (Basel), 2019; 8(2):30. CrossRef
Zadka K, Pa?kowska-Go?dzik E, Roso?owska-Huszcz D. The state of knowledge about nutrition sources of vitamin D, its role in the human body, and necessity of supplementation among parents in Central Poland. Int J Environ Res Public Health, 2018; 15(7):1489. CrossRef
Zarooni AAR, Marzouqi FIA, Darmaki A, Prinsloo EAM, Nagelkerke N. Prevalence of vitamin D deficiency and associated comorbidities among Abu Dhabi Emirates population. BMC Res Notes, 2019; 12(503):1–6. CrossRef