
INTRODUCTION
Nigeria has the second-largest Human Immunodeficiency Virus (HIV) epidemic in the world (UNAIDS, 2017). The South–South zone of the country (where Akwa Ibom State is located) has the highest prevalence of the disease with statistical values of 5.5% for the South-South zone and 6.5% for Akwa Ibom State. This means that Akwa Ibom is one of the states in Nigeria where the disease is endemic (NACA, 2015). The prevalence of the infection in Akwa Ibom State was somehow relatively high for the period 2001–2010 with the values being 10.7% in 2001, 8.0% in 2005, and 10.9% in 2010 (Bashorun et al., 2014). However, the prevalence in the state has reduced to 6.5% by the end of 2015 due to multiple approaches of the disease control (NACA, 2015).
The control of HIV infection using antiretroviral therapy (ART) has led to a significant reduction in the transmission, morbidity, and mortality of the infection (WHO, 2016). Pharmacists are contributing significantly to HIV/AIDS care and research (Horace, 2012). Until recently, the clinic-based model was the mainly promoted approach to disease control. The community-based approach was introduced as a means of reaching out to the large pool of the unreached infected people. It started in the form of house-to-house testing. Community pharmacists in Nigeria have shown willingness to provide HIV/AIDS care (Ajagu et al., 2017).
In July 2014, the Joint United Nations Programme on HIV and AIDS (UNAIDS) called for a global scale-up of treatment as an effort to meet the 90-90-90 target by 2030 (UNAIDS, 2014). As more people are being placed on treatment, the existing care facilities are getting over-crowded. Antiretroviral service delivery at community pharmacy presently known as community pharmacy antiretroviral refill programme (CPARP) was introduced to relieve the treatment site.
Community Pharmacy Antiretroviral Refill Programme is a new community-based model. It was introduced in Akwa Ibom State in October 2016. In this program, stable clients are devolved from hospitals and clinics to some selected community pharmacies for medication refill (Avong et al., 2018). A stable HIV/AIDS patient, according to this program, is one who has been on ART for not less than 1 year, has a viral load of less than 1000 cells/mL, not a defaulter in term of medication adherence, and does not have a current opportunistic infection. In addition, the client must be on first-line agents and willing to be so devolved to the community pharmacy.
After being devolved, the client receives medication from the pharmacy every quarter; and returns to the clinic every 6 months for clinical assessment (Fhi 360, 2016). Laboratory evaluation (viral load determination) is also carried out at the clinic every 6 months for the first 12 months then every year subsequently. The services provided at the community pharmacies for the clients include chronic care screening, medication adherence monitoring, antiretrovirals (ARV) refill, counseling and support, documentation, referral, and linkages (Cocohoba et al., 2012; Hirsch et al., 2011; Murphy et al., 2012).
Differentiated care holds the promise of improving the efficacy of service delivery as well as increasing clients’ satisfaction. While achieving the intended objectives of CPARP (which include decongestion of the clinics to allow for better quality time for unstable and new clients as well as provision of differentiated care for the stable and willing clients at community pharmacy), the satisfaction of the devolved clients must be ensured. This work is aimed at assessing antiretroviral service delivery at selected community pharmacies in Akwa Ibom State, Nigeria.
METHODS
Study population/setting
The study was carried out at three community pharmacies rendering anti-retroviral refill services in Akwa Ibom State, Nigeria. Nigeria, for administrative purposes, is divided into 36 states with each state further divided into Local Government Areas. Within each state, all the Local Government Areas are grouped into three senatorial districts. Akwa Ibom State is located at the South-South zone of Nigeria and consists of three senatorial districts, namely, North-West (Ikot-Ekpene), North-East (Uyo), and South (Eket) districts. At the onset of this research, CPARP was available at 25 community pharmacies across eight Local Government Areas spread over the three senatorial districts. The total number of clients receiving ARV refill at community pharmacies in the state at that moment was 1,157.
Study design
A systematic cross-sectional study was used. The Howard University Global Initiative Nigeria was contacted to know the community pharmacy with the largest number of devolved HIV clients in each of the three senatorial districts of Akwa Ibom state. The three pharmacies were selected for the study. The selected pharmacies were coded A, B, and C: Pharmacy “A” at Ikot-Ekpene (North-West district), Pharmacy “B” at Uyo (North-East district), and Pharmacy “C” at Oron (Southern district).
The study sample consisted of clients receiving refill from the three community pharmacies. The exclusion criterion is those who have not spent up to 6 months in receiving refill at the community pharmacy. The sampling was done within the 3 months of July, August, and September 2018. It was done such that nobody is sampled twice as the clients receive their medication once in 3 months.
Ethical issues
Clients’ consents were sought at the introductory part of the questionnaire. The ethical approval for the study was obtained from Akwa Ibom State Ministry of Health, Uyo, Nigeria (Reference number MH/PRS/99/Vol. IV/277).
Study instrument
The instrument used for the study was a pre-tested questionnaire containing questions to obtain socio-demographical data, medical and pharmaceutical data, devolvement information, quality of services received at the pharmacies, clients’ satisfaction level, and the likelihood of recommending the program for prospective clients. Two hundred and twenty-five copies of the questionnaire were produced and 75 copies were given to each of the superintendent pharmacists of the three selected community pharmacies.
The questionnaire was divided into five sections. Section 1 comprised eight questions on socio-demographic characteristics of the participants; Section 2 comprised five questions on medical and pharmaceutical data of the participants, while Section 3 comprised four questions on reasons for accepting devolvement. Section 4 comprised four questions on the effectiveness of the community pharmacy ARV refill program and Section 5 comprised two questions on the level of clients’ satisfaction.
Data collection
Pharmacists who were involved in the antiretroviral refill for the patients were used for the data collection as they have adequate knowledge of the work being done. The participants were notified of the purpose of the study. Data were collected from the participants in the form of completion of the questionnaire when they came for their refill within the 3 months of the study. The completed questionnaires were collated by the pharmacists-in-charge and handed over to the investigator.
Outcome measured
The outcomes measured were: socio-demographical data of clients, medical and pharmaceutical data, devolvement information, quality of services received at the pharmacies, and clients’ satisfaction level (including the likelihood of recommending the program for prospective clients).
Data analysis
Some data collected were expressed as proportions while others were expressed graphically. Analysis was done using the Chi-squared test and level of significance was set at p values < 0.05.
RESULTS AND DISCUSSION
Socio-demographic characteristics of participants
Fifty-one questionnaires were completed and returned at Ikot-Ekpene, 49 at Uyo, and 75 at Oron giving a total of 175. The socio-demographic characteristics of the participants are shown in Table 1.
The number of participants who were single and the number who were married were not significantly different for Ikot-Ekpene. Majority of the participants from Uyo and Oron were married. Most of the participants were not only within the reproductive age, but they were also married. Oron had the highest proportion of participants that were widowed. Oron local government has a high incidence of the disease and would have had more mortality compared to the other districts.
All the participants from Ikot-Ekpene and Uyo; and 97.33% of those from Oron were Christians. The prevalent level of education of participants from each district is a reflection of the type of settlement. Uyo is more of urban compared to Ikot-Ekpene compared to Oron. Hence, the prevalent level of education among the participants from Uyo, IKot Ekpene, and Oron was tertiary, secondary, and primary, respectively. Secondary education had the highest frequency for Ikot-Ekpene, tertiary education had the highest frequency for Uyo while primary education had the highest frequency for Oron.
Medical and pharmaceutical data
The proportions of participants having a viral load of less than 20 cells/ml were 92.16%, 77.55%, and 57.33% for Ikot-Ekpene, Uyo, and Oron, respectively. All the participants had a viral load below 1,000 cells/ml which is the benchmark for devolvement. Hence, they are all virologically controlled. This is a pointer to the effectiveness of the antiretroviral service delivery at community pharmacies in Akwa Ibom State.
The proportion of the participants on different ARV combinations and opportunistic infection prophylaxis are shown in Table 2.
There was no significant difference in the number of clients on Tenofovir/Lamivudine/Efavirenz (TDF/3TC/EFV) and those on Zidovudine/Lamivudine/Nevirapine (ZDV/3TC/NVP) for Ikot-Ekpene. ZDV/3TC/NVP had the highest frequency for Uyo while TDF/3TC/EFV had the highest frequency for Oron. One of the criteria for devolvement is that the client must be stable on first-line ARVs. All the clients were on TDF/3TC/EFV or ZDV/3TC/NVP or Abacavir/Lamivudine/Efavirenz (ABC/3TC/EFV). Hence, all the clients were still being maintained on the first-line agents.
Some of the clients were placed on both cotrimoxazole and Isoniazid prophylaxis, some on cotrimoxazole only while some others on isoniazid only. Participants from Ikot-Ekpene were better protected against opportunistic infections compared to the other districts. Most of the participants from Uyo were not given prophylaxis for opportunistic infections.
Most deaths from HIV/AIDS are from opportunistic infections (Benson et al., 2004). Prominent among these infections are tuberculosis, toxoplasmosis (Toxoplasma gondii encephalitis), Salmonella and Shigella gastroenteritis and Pneumocystis jiroveci pneumonia. Isoniazid is administered in conjunction with the ARVs as prophylaxis for tuberculosis while co-trimoxazole is administered as prophylaxis for the other bacterial infections.
From Table 2, it can be said that all the participants from Ikot Ekpene are protected from the typical bacterial infections while only 11.76% are protected from mycobacterial infection. Only 34.69% of the participants from Uyo are protected from the typical bacterial infections while 2.04% are protected from tuberculosis. In the case of Oron, 92% of the participants are protected from the typical bacterial infections while 8% are protected from tuberculosis.
 | Table 1. Sociodemographic characteristics of the participants (N = 175). [Click here to view] |
 | Table 2. Medical and pharmaceutical data of participants. [Click here to view] |
Reasons for accepting devolvement
The reasons for which the participants accepted devolvement are shown in Figure 1. The proportions of the participants who agreed to different points as being one of the reasons they accepted devolvement were represented by the chart.
All the participants from Uyo and Oron districts indicated “better privacy” and “shorter waiting time” as reasons for accepting devolvement; all the participants from Uyo district indicated “flexible drug pick-up” as a reason for accepting devolvement while “proximity to place of residence” had the lowest frequency for all the districts. Hence, “better privacy” and “shorter waiting time” are the two most significant factors for accepting devolvement while “proximity to residence” is the least significant.
General hospital Oron and University of Uyo teaching hospital have the highest enrollments for HIV/AIDS care in Akwa Ibom State. Hence, there is pressure on these facilities and the quality of the services rendered might be affected. A vast majority of the participants from the districts where these facilities are located indicated most of the four reasons as to why they accepted devolvement.
“Waiting time” as the most significant of all the reasons is due to the high burden on the hospitals. “Proximity to residence” being the least significant can be attributed to the fact that the participants are based at different areas and the hospitals may be close to some and be far from others; the same condition is applicable to the location of the community pharmacies.
Efficiency and effectiveness of the community pharmacy ARV refill programme
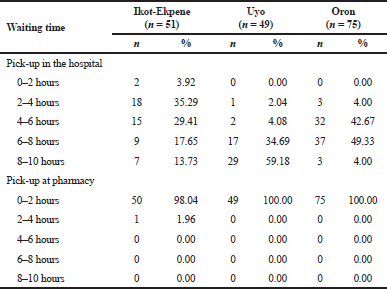
The average waiting times during drug pick-up at the hospital and at the community pharmacies are shown in Table 3. For drug pick-up at the hospitals, the range 4–6 hours is the median pick-up time for Ikot Ekpene, 8–10 hours is the median for Uyo, and 6–8 hours is the median for Oron; while for pick-up in community pharmacy, 98.04% to 100% of the participants reported 0–2 hours as the waiting time for all the districts.
Comparing waiting time at the hospital with that of community pharmacy, there is 300% reduction in waiting time for Ikot Ekpene, 500% reduction for Uyo, and 400% reduction for Oron. This corresponds to the initial observation that shorter waiting time is the most significant reason for accepting devolvement.
.png) | Figure 1. Proportions of participants who agreed to different points as a reason for accepting devolvement. [Click here to view] |
 | Table 3. Waiting times during drug pick-up. [Click here to view] |
 | Table 4. Effectiveness of the community pharmacy ARV refill. [Click here to view] |
 | Table 5. Level of clients’ satisfaction. [Click here to view] |
 | Figure 2. Likelihood of clients recommending community pharmacy ARV refill programme for their colleagues. [Click here to view] |
The services, provided by the community pharmacists for the clients included chronic care screening, medication adherence monitoring, ARV refill, counseling and support, and documentation. The proportions of participants who received different services during drug pick-up in the community pharmacies are shown in Table 4. The attitudes of the participants (clients) and those of the pharmacists in situations where the clients missed appointments are also shown in Table 4. Table 4 shows that the clients were given adequate pharmaceutical services. The attitudes of the clients and those of the pharmacists as well as the use of fixed-dose combination therapy are indications that there was a high level of adherence. This is in agreement with the work of Cocohoba et al. (2012) carried-out at California Walgreens Pharmacies which showed that the use of fixed-dose combination therapy promotes adherence.
Level of clients’ satisfaction
The proportions of clients showing different levels of satisfaction with respect to the services received at the community pharmacy are shown in Table 5.
For Ikot-Ekpene district, a total of 94.12% of the participants were satisfied (moderately and highly) with chronic care screening, 96.08% were satisfied (moderately and highly) with medication adherence monitoring, 88.24% were satisfied (moderately and highly) with ARV refill, 88.24% were satisfied (moderately and highly) with counseling and support while 92.16% were satisfied (moderately and highly) with the entire program. For Uyo, all the participants were satisfied (moderately or highly) with chronic care screening, medication adherence counseling, ARV refill, counseling and support, and the entire program. For Oron, all the participants were highly satisfied with the individual services received and with the entire program.
The likelihood of clients recommending the program for their colleagues is illustrated in Figure 2. For all the districts, no client indicated “very unlikely” nor “unlikely” in respect of recommending the program. “Very likely” had the highest frequency for all the districts.
The high level of satisfaction of the participants with all the aspects of the program is a reflection of the success of the program. Some of the reasons for introducing the CPARP are: to make the refill sites closer to the clients, save time, decongest the treatment sites and pave way for the care for new clients. The observation from this study shows that these targets are attainable, with the participants showing their willingness to recommend the program for their colleagues.
CONCLUSION
Clients receiving antiretroviral services at the community pharmacies are well controlled using the first-line ARVs. “Shorter waiting time” is the most prevalent reason for accepting devolvement while “proximity to residence” is the least prevalent reason. Clients do not spend up to 2 hours in community pharmacy before receiving pharmaceutical care; and the services received by clients include: chronic care screening, medication adherence monitoring, ARV refill, counseling, and support. Antiretroviral service delivery at community pharmacy is successful in Akwa Ibom state; and benefitting-clients are very likely to recommend the program for their colleagues who have yet to be devolved. Isoniazid preventive therapy should always be made available to eligible clients. It is hereby recommended that similar studies be carried out in other States to see whether similar results will be obtained. Also, epidemiological studies of HIV can be carried out after some years of introducing CPARP in Akwa Ibom State to determine the effect of the program on the prevalence of the disease.
AUTHORS’ CONTRIBUTIONS
Emmanuel O. Olorunsola was involved in the conception of the work, the design, data analysis, and drafting of the manuscript; Florence E. Eichie was involved in the design of the work, data interpretation, and initial revision of the manuscript for intellectual content while Sunday O. Awofisayo was involved in the data collection, analysis, and initial revision of manuscript for intellectual content. All the authors gave final approval of the version of the manuscript being published.
CONFLICTS OF INTEREST
There are no competing interests regarding the publication of this paper.
ACKNOWLEDGMENT
The authors are grateful to Pharmacists Chidiebere Joseph Ariasike, and Lovina Etido Essiet for helping in the data collection using the questionnaire.
REFERENCES
Ajagu N, Anetoh MU, Ndukka SO. Expanding HIV/AIDS care service sites: a cross-sectional survey of community pharmacists’ view in South-East, Nigeria. J Pharm Policy Pract, 2017; 10(34):1–12. CrossRef
Avong YK, Aliyu GG, Jatau B, Gurumnaan R, Danat N, Kayode GA, Adekanmbi V, Dakum P. Integrating community pharmacy into community based anti-retroviral therapy program: A pilot implementation in Abuja, Nigeria. PloS One, 2018; 13(1):e0190286. CrossRef
Bashorun A, Nguku P, Kawu I, Ngige E, Ogundiran A, Sabitu K, Nasidi A, Nsubuga P. A description of HIV prevalence trends in Nigeria from 2001 to 2010: what is the progress, where is the problem? Pan Afr Med J, 2014; 18(Suppl 1): Article 3. CrossRef
Benson CA, Kaplan JE, Masur H, Pau A, Holmes KK. Treating opportunistic infections among HIV-exposed and infected children: recommendations from CDC, the National Institutes of Health and the Infectious Disease Society of America. Morbid Mortal Wkly Rep, 2004; 53:1–112.
Cocohoba JM, Murphy P, Pietrandoni G, Guglielmo BJ. Improved antiretroviral refill adherence in HIV-focused community pharmacies. J Am Pharm Assoc, 2012; 52:67–73. CrossRef
Fhi 360 (Family Health International). A synopsis of differentiated care for ART programme managers, 2016. Available via (Accessed 27 December 2017).
Horace AE. Pharmacists’ research contributions in the fight against HIV/AIDS. AIDS Res Treatm, 2012; Article 869891:1–5. CrossRef
Hirsch JD, Gonzales M, Rosenquist A, Miller TA, Gilmer TP, Best BM. Antiretroviral therapy adherence, medication use, and health care costs during 3 years of a community pharmacy medication therapy management program for Medi-Cal beneficiaries with HIV/AIDS. J Managed Care Pharm, 2011; 17:213–23. CrossRef
Murphy P, Cocohoba J, Tang A, Pietrandoni G, Hou J, Guglielmo BJ. Impact of HIV-specialized pharmacies on adherence and persistence with antiretroviral therapy. AIDS Patient Care STDs, 2012; 26:526–31. CrossRef
NACA (National Agency for the Control of AIDS). Nigeria: Global AIDS Response Country Progress Report, 2015. Available via https://naca.gov.ng (Accessed 26 December 2017).
UNAIDS (Joint United Nations Programme on HIV and AIDS). Joint United Nations Programme on HIV/AIDS 90-90-90: an ambitious treatment target to help end the AIDS epidemic, 2014. Available via www.unaids.org (Accessed 27 December 2017).
UNAIDS (Joint United Nations Programme on HIV and AIDS). UNAIDS Data book, 2017. Available via (Accessed 26 December 2017).
WHO (World Health Organization). Consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection. Available via http://wwwwhoint/hiv/pub/arv/arv-2016/en/ (Accessed 28 October 2018).